

Behavioral health needs continue to outpace available resources, especially among Medicaid-enrolled populations served by Federally Qualified Health Centers (FQHCs) and Community Mental Health Centers (CMHCs). Patients often face fragmented care, long wait times for psychiatric services, and challenges managing comorbid physical and mental health conditions.
The collaborative care model (CoCM) offers a proven, evidence-based solution. This team-based approach integrates psychiatric expertise into primary care and other medical settings, improving access, outcomes, and efficiency while creating sustainable reimbursement pathways.
For facilities serving high volumes of Medicaid patients—like FQHCs and CMHCs—CoCM aligns perfectly with mission-driven care and opens doors to enhanced revenue through dedicated billing codes.
FasPsych, a leader in telepsychiatry and behavioral health staffing, helps organizations implement and scale this model effectively.
What Is the Collaborative Care Model (CoCM)?
The collaborative care model is a specific, highly structured form of integrated behavioral health care. It embeds mental health support directly into primary care or similar settings through a small, proactive team rather than relying on traditional referrals to specialty psychiatry.
Developed at the University of Washington and refined through decades of research (including the landmark IMPACT trial), CoCM uses measurement-based care, population health principles, and regular psychiatric consultation to treat common conditions like depression, anxiety, and comorbid chronic illnesses.
Core Team Members
- Primary Care Provider (PCP) or Treating Clinician: Leads overall care, prescribes medications when appropriate, and directs the team.
- Behavioral Health Care Manager (BHCM): Typically a licensed clinical social worker, nurse, or trained mental health professional. Handles patient engagement, brief evidence-based interventions (e.g., behavioral activation or problem-solving therapy), tracks progress via a registry, and coordinates care.
- Psychiatric Consultant: A psychiatrist (or psychiatric nurse practitioner in some models) who provides caseload-focused consultation—often via telehealth—reviewing the registry regularly (e.g., weekly) and offering medication recommendations or treatment adjustments without needing to see every patient directly.
This structure allows one psychiatrist to meaningfully support hundreds of patients across multiple sites.
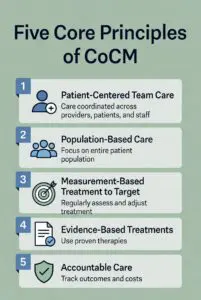
The Five Core Principles of the Collaborative Care Model
Effective CoCM requires fidelity to these principles (developed with input from national experts and supported by the AIMS Center at the University of Washington):
- Patient-Centered Team Care: Shared care plans incorporate patient goals; care feels seamless in one familiar setting.
- Population-Based Care: A defined patient registry tracks everyone on the caseload so no one falls through the cracks; proactive outreach targets those not improving.
- Measurement-Based Treatment to Target: Use validated tools (e.g., PHQ-9 for depression, GAD-7 for anxiety) at regular intervals; adjust treatment until clinical goals are met (stepped care approach).
- Evidence-Based Treatments: Offer proven interventions, including brief psychotherapy and medications, tailored to primary care.
- Accountable Care: Track quality metrics and outcomes for continuous improvement; reimbursement ties to results in many value-based models.
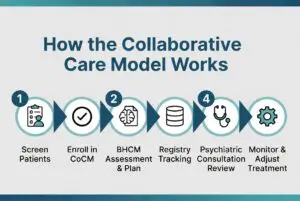
How CoCM Works in Practice
- Screen patients in primary care or the medical home setting.
- Enroll consenting patients meeting criteria into the CoCM program.
- BHCM engages the patient, conducts initial assessment, develops a plan, provides brief interventions, and enters data into the registry.
- Psychiatric consultant reviews the caseload systematically and provides recommendations.
- Team monitors progress with measurements; steps up care or refers to specialty services as needed.
- Prepare for discharge/relapse prevention when goals are achieved.
The model emphasizes efficiency: most psychiatric input happens through consultation rather than direct visits, dramatically expanding access.
Evidence and Benefits:
- Over 80 randomized controlled trials and meta-analyses show CoCM doubles improvement rates for depression compared to usual care and improves outcomes for comorbid conditions.
- Better access, reduced stigma, higher patient/provider satisfaction.
- Cost-effective: Often cost-neutral or savings-generating through fewer ED visits and hospitalizations.
- Scalable workforce solution amid psychiatrist shortages.
Learn more from the authoritative source: AIMS Center Collaborative Care resources.
CoCM Billing Codes and Reimbursement Impact
Dedicated CPT/HCPCS codes (introduced by CMS and adopted widely) reimburse the care management and consultation work that was previously unbillable or bundled. Key codes include:
- 99492: Initial month (first 70 minutes of BHCM activities).
- 99493: Subsequent months (first 60 minutes).
- +99494: Add-on for each additional 30 minutes.
- G2214: Shorter 30-minute option for any month.
- For many FQHCs/RHCs: G0512 (composite or specific psychiatric CoCM code, often with PPS encounter rate add-ons in some states).
Time thresholds apply (CPT time rule for most settings: midpoint +1 minute), with documentation of registry use, psychiatric consultation, measurements, and interventions required. Patient consent (verbal often suffices) and an initiating visit are typically needed.
How this improves facility reimbursement:
- Creates predictable monthly per-patient revenue on top of standard E/M or encounter visits.
- Supports hiring or contracting BHCMs and psychiatric consultants.
- Many Medicaid programs, Medicare, and commercial payers cover these codes (with state variations; FQHCs often bill G0512 or individual codes plus their prospective payment system rate).
- In value-based or shared-savings arrangements, better outcomes can yield additional bonuses.
- Helps offset costs in high-Medicaid environments where traditional fee-for-service psychiatry reimbursement can be challenging.
Facilities report strong ROI when implementation includes proper workflows, training, and time tracking.
For billing information, explore the American Psychiatric Association’s Integrated Care tools.
Why the Collaborative Care Model Excels for Medicaid Patients in FQHCs and CMHCs
FQHCs and CMHCs serve large Medicaid populations with complex needs: higher rates of chronic conditions, social determinants of health challenges, trauma, and barriers to specialty care (especially in rural or underserved areas). Traditional models often result in long waits or lost follow-up.
CoCM addresses these challenges effectively:
- Improved Access and Equity: Brings psychiatric expertise into the medical home via telepsychiatry consultation—ideal for rural FQHCs or CMHCs with limited on-site psychiatrists. Patients receive care where they already go for primary or behavioral health services, reducing stigma and transportation barriers.
- Holistic, Integrated Care: Aligns with FQHC mission of comprehensive services and CMHC focus on community-based treatment. Handles comorbid physical/mental health and supports whole-person approaches including SDOH considerations.
- Measurement-Driven Outcomes: Registry and regular tracking help demonstrate value to payers and improve quality metrics tied to Medicaid contracts or value-based payments.
- Workforce Efficiency: Psychiatric consultants (via telehealth) support larger caseloads without proportional hiring increases—critical amid shortages.
- Financial Sustainability: Billing codes provide dedicated revenue streams. Many states’ Medicaid programs reimburse CoCM (fee-for-service or managed care), and FQHCs can often combine with PPS rates. This helps facilities move beyond grant dependency toward sustainable operations.
- Reduced Fragmentation and Better Continuity: Team-based approach with shared plans minimizes patients falling through cracks, lowers readmissions, and supports transitions of care.
- Scalability for High-Volume Settings: Works well in busy clinics; BHCM handles day-to-day coordination while consultants provide high-level oversight.
Real-world adaptations show strong results in safety-net settings. Telepsychiatry integration further enhances reach for Medicaid populations.
How FasPsych Supports CoCM in Your Facility
 Implementing or expanding the collaborative care model requires reliable psychiatric consultation, flexible staffing, compliance expertise, and seamless integration with your workflows and EHR. FasPsych specializes in exactly this.
Implementing or expanding the collaborative care model requires reliable psychiatric consultation, flexible staffing, compliance expertise, and seamless integration with your workflows and EHR. FasPsych specializes in exactly this.
As a trusted telepsychiatry partner, FasPsych provides:
- Board-certified psychiatrists and psychiatric nurse practitioners for caseload consultation and medical direction.
- Customizable models (remote, hybrid, or on-site as needed) tailored to FQHCs, CMHCs, primary care, and other Medicaid-focused settings.
- Support for integrated care teams, including collaboration with your BHCMs and PCPs.
- HIPAA-compliant platforms, documentation integration, and e-prescribing.
- Flexible engagement: full-time equivalents, part-time, PRN, or consultative hours—pay only for what you use.
- Expertise in serving diverse organizations, including those with high Medicaid volumes.
FasPsych helps facilities leverage CoCM’s clinical and financial benefits without the burden of recruiting scarce psychiatric talent in-house.
Explore how we support primary care and integrated settings: FasPsych Primary Care Providers page.
See related insights on our blog: Integrated Care Model Implementation Guide for PCPs and Psychiatrists in Integrated Care Teams.
Ready to Improve Care and Reimbursement with the Collaborative Care Model?
The collaborative care model delivers better outcomes for patients, stronger support for your clinical teams, and enhanced financial sustainability—particularly valuable for FQHCs, CMHCs, and other facilities serving Medicaid populations.
FasPsych makes implementation practical and scalable through expert telepsychiatry psychiatric consultation and staffing solutions.
Contact FasPsych today to discuss how we can partner with your organization:
- Visit: https://faspsych.com/partner-with-us/
- Call: (877) 218-4070 or (480) 970-9097
- Explore services: https://faspsych.com/telepsychiatry-services/
Let’s work together to bring high-quality, integrated behavioral health care to more patients while strengthening your facility’s operations and reimbursement. Reach out now for a consultation tailored to your needs.